

- 赖红昌教授
- 上海九院口腔种植科主任
- 口腔种植支持固定修复
- 口腔种植支持活动修复等
上海九院种植牙口腔颅颌面种植科主任,教授、主任医师、博士生导师。现任中华口腔医学会口腔种植专业委员会主任委员,国际口腔种植协会专家委员会委员...[详细]
研究成果


种植体单冠修复的美学效果及软组织改变
更新时间:2019-06-27 14:35
种植体单冠修复的美学效果及软组织改变 :一项2年前瞻性研究
Esthetic outcome and alterations ofsoft tissue aroundsingle implantcrowns: a 2-year prospective study
倪杰 翻译;王刃 审校
关键词 : 种植体,粉红美学评分/白色美学评分, 软组织美学效果, 组织水平
摘要
目的 : 这项前瞻性研究旨在评估组织水平种植牙的美学效果和周围软组织变化,以及植骨与牙龈生物型对其影响。
材料与方法 : 对上颌前牙区单牙缺失的38名患者植入Straumann Standard PlusSLA植体,其中24名患者进行了骨增量手术,戴冠后12及24个月对这些患者进行随访。评估分析粉红美学评分/白色美学评分(PES/WES)以及各项临床指标。
结果 : 在戴冠后2天(基线)、戴冠后1年和2年种植体周围的平均PES/WES值分别是13.79、 14.87和14.96。戴冠后1年和基线相比PES/WES值有显著提高(P<0.01)。但在1年和2年之间,两值的提高不显著(P=0.40)。在戴冠后2年,厚龈生物型患者平均PES改变要显著高于薄龈生物型患者(P=0.03)。植骨手术在基线及后期随访中有不利于平均PES值的效果(P<0.01)。 2年的随访中没有种植体失败, 3名患者有种植体周围感染。这段时间的改良菌斑指数(mPI),牙周袋探诊深度(PPD)和改良出血指数没有显著差异。
结论 : 根据本前瞻性研究,在美学区用软组织水平种植体修复单牙缺失病例是可行的。不论植骨与否,种植体单冠周围美学效果和软组织稳定性在短期之内都可以达到满意的结果。然而,植骨手术也许对美学效果有不利影响。牙龈生物型也许可以考虑成为美学效果预后影响因素。软组织水平种植体系统对种植体周软组织稳定性的影响还需要长时间随访的随机对照临床试验提供证据。
近年来,高存留率和成功率使牙种植体成为修复单牙缺失间隙的常规手段(Pjetursson et al.2007, 2012;Jung et al.2008)。然而,种植治疗的成功不能仅仅局限于骨结合,修复后的美学效果也应当成为临床病例成功的重要参考因素,特别是对于一些美学要求较高的病例。
评估种植牙的临床美学效果应当考虑种植体牙冠特征和种植体周软组织的稳定性(Chang et al.1999),而种植体周围软组织美学是临床处理的难点。种植美学失败的最常见原因包括粘膜颜色或者质地的不协调,牙间乳头完全或不完全丧失,以及软组织的退缩。因此想要达到临床美学成功,软组织美学效果至关重要(Belser et al.2004)。
目前越来越多的研究采用粉红美学评分(PES)(Furhauser et al.2005)或者结合粉红美学评分/白色美学评分(PES/WES)(Belser et al.2009)来评估种植牙美学效果和周围软组织的变化。大约三分之一的I型种植术患者(拔牙后即刻种植)为了达到PES得分的稳步提升需要进行结缔组织移植(Cosyn et al.2013),而对于II型(拔牙后4~8周)和III型(拔牙后12~16周)种植术患者,短期内PES得分也许会自然而然的提高,但当观察时间延长到正式冠戴入后三年以上,其PES得分可能就会返回到基线水平(Buser et al.2011, 2013; Weinlander et al.2011; Pieriet al.2013)。
值得一提的是以上各研究所采用的一律只有骨水平种植体系统。因其简单的手术程序和平台转移技术应用所带来的更少的骨吸收,骨水平种植体现广泛的被应用于美学区牙列缺损病例(Al-Nsour et al.2012;Annibaliet al.2012)。
与此同时,软组织水平种植体系统也被广泛应用于临床,但几乎没有相关研究报道软组织水平种植体系统的美学评价。在我们研究小组先前已发表的文章当中,已证实在精确控制植入种植体深度的前提下,软组织水平系统也能达到可预期的软组织形态(Lai etal. 2008)。然而,该研究随访时间相对较短(6~8月),且没有纳入需要植骨的病例。据我们所知,本研究是第一项关于用软组织PES指数评价包括进行骨增量手术患者及未进行骨增量手术患者的软组织水平种植体的前瞻性研究。
因此,本研究的目的是 :一,评估2年随访期间软组织水平种植体周围美学效果和软组织改变。二,研究对种植体周围软组织的美学效果的影响因素,包括植骨和牙龈生物型。
材料与方法
研究设计和患者数据
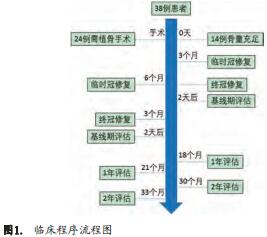
本研究是一项在上海市第九人民医院口腔颌面种植科进行的经2年随访的前瞻性研究。从2010年5月至2012年5月,纳入40名年龄从19~58岁(平均31.3岁)全身状况健康的患者(18名女性, 22名男性),术前均签署知情同意书,并对所有患者进行口腔卫生指导。图1为临床程序流程。纳入标准如下 :
1. 上前牙区单牙缺失需要修复的患者。
2. 术前至少已经拔牙三个月以上。
3. 无严重的垂直骨缺损,有足够的初期稳定性保证种植体同期植入。
4.非重度吸烟者(>10支/天)。
5.邻牙无修复治疗需要者。
处理
种植体植入
本研究所用的种植体都是Straumann Standard Plus SLA植体(Institut Straumann AG, Waldenburg, Switzerland),根据术前临床及影像学检查设计种植手术。按照Buser等(Buser et al. 2004)描述的种植体三维位置植入植体,如果种植体颈部暴露或颊侧骨板厚度小于1 mm,则需要进行骨增量手术。用自体骨加去蛋白牛骨颗粒(Bio-Oss 0.25–0.5 mg, Geistlich Biomaterials, Wolhusen,Switzerl)覆以胶原膜(Bio-Gide 25*25 mm, Geistlich Biomaterials)修复骨缺损,并用Ethilon5-0尼龙线缝合切口。
愈合阶段
手术后,患者使用消炎药阿莫西林(新亚Co,上海,中国, 500毫克,每天四次,7天)和甲硝唑(信谊万象,上海,中国, 400毫克,每天三次,7天)。此外,用0.12%洗必泰漱口60秒,每天5到6次,持续14天。在愈合期间,使用不干扰伤口愈合的可摘局部义齿,术后7~10天拆线。
修复阶段
术后3~6月进行上部修复,必要时行二期手术,根据印模帽形态制作临时塑料冠(图2)。患者每月复诊,根据软组织边缘调整塑料冠,三个月后,种植体水平取模,制作烤瓷单冠修复体。

结果指标
美学评价
种植体周围软组织的评估在修复体戴入后2天(作为基线)由两位正畸医师用PES/WES分别独立评分。临床照片由一名护士用单反相机完成(D70, Nikon, Tokyo, Japan)。 在基线,1年及2年随访时拍照,拍摄的照片需要包含两边至少各有一个天然邻牙。两名正畸医师用2-1-0评分系统填写含有10个指标的表格来评估软组织和修复体美学效果,并计算平均值和频率。根据总分可分为三个等级 :好级(PES≥9),可接受级(9>PES≥6),不理想级(PES<6)(Belseret al. 2009; Cosyn et al. 2012)。
临床评价
存留率被定义为种植体仍存在在口腔当中的百分率。所有生物学和机械并发症都被记录,另外,以下临床指标也需要记录 :牙龈生物型(Muller et al. 2000),改良菌斑指数(mPI),牙周探诊深度(PPD),改良出血指数(mBI)。以上所有测量都由同一位牙医用牙周探针完成 (15 UNC/CP-11.5BScreening Color-Coded Probe, HuFriedy)(Mombelli et al. 1987).
随访
患者需要于戴牙后1年和2年后复诊进行美学和临床评估, mPI、 PPD、 mBI和PES/WES等指数在随访中被记录。
统计学方法
用统计软件包STATA(version 11.0;StataCorp, College Station, TX, USA)进行数据分析。用Wilcoxon符号秩检验分析非正态分布数据(mBI, mPI, PPD和PES/WES)。用组内相关系数确定检查者间的可靠性。用Wilcoxon秩和检验分析平均PES值并比较植骨或非植骨手术病例及不同牙龈生物型患者间的的PES值的异同。 P值为双尾,设定5%为具有统计学意义。
结果
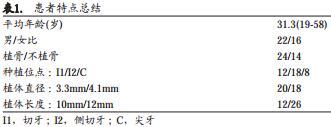
2年随访后, 2名患者因不能继续按期随访而被排除,最终38名患者被纳入到分析当中。表1显示所有患者的人口学特征。
两名正畸医师给出的平均PES/WES值得到的组内相关系数在基线为0.85,在戴冠后1年和2年均为0.82。
表2显示的是从基线到1年随访的平均PES/WES值,第一年随访PES/WES从13.79显著增加到14.87 (P<0.01)。具体而言, 1年随访的近、远中龈乳头,软组织边缘弧度以及PES的均值有显著增加。此外,软组织边缘水平,根部突度/颜色/质地的平均值略有增加,但都没有统计学意义。
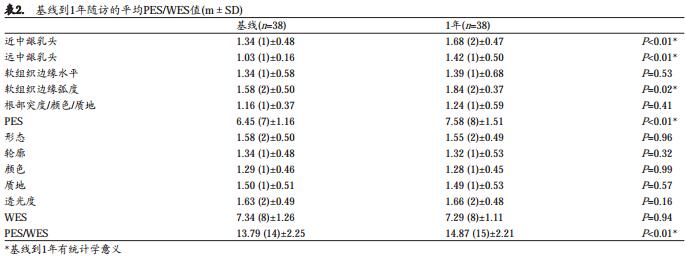
表3显示的是从1年随访到2年随访的平均PES/WES值。到第二年随访, PES/WES值的提升仍然稳定(从14.87到14.96, P=0.40)。具体来说,近、远中龈乳头,软组织边缘弧度,根部突度/颜色/质地以及PES均值的提升都十分稳定。软组织边缘水平均值略减少。 1年到2年的随访期间没有指标显示出具有统计学意义的不同。图3为本研究中较典型的病例。
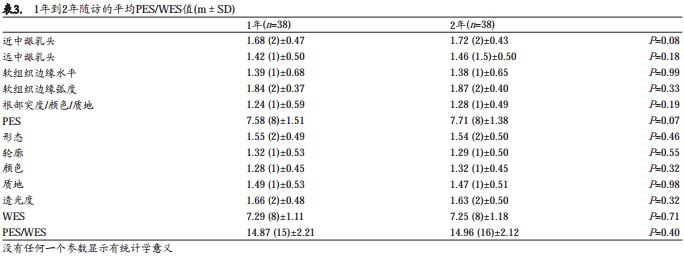
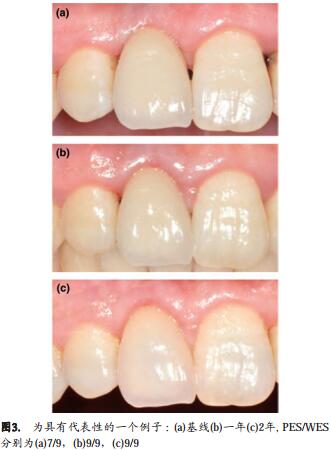
表4显示的是在基线、 1年、 2年随访的PES频率。2年间,好级(PR)从2.63%提升到34.21%,可接受级(AR)从78.95%降到59.21%,不理想级(UR)从18.42%降到6.58%。
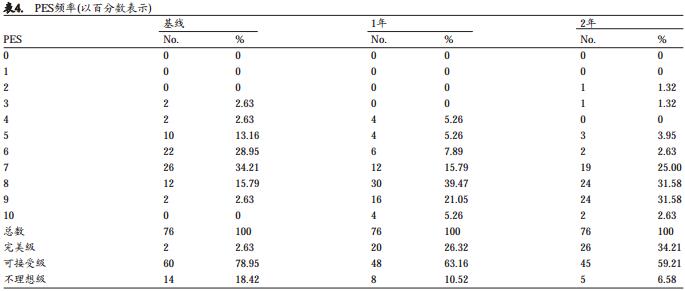
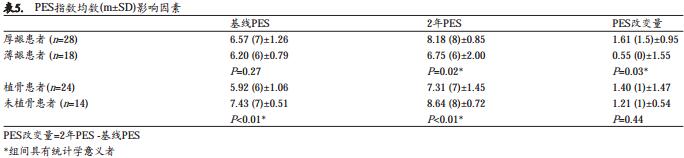
表5显示的是种植体周围软组织美学效果受不同变量的影响。在基线时,薄龈型患者与厚龈型患者的平均PES值没有很显著的差异(P=0.27)。然而,厚龈型患者在后期随访中能够达到显著更高的PES均值(P=0.02)。此外,厚龈型患者PES改变值会更高(P=0.03)。植骨手术对于基线和后期随访的平均PES值显示不良效果(P<0.01)。然而,植骨患者与不植骨患者具有类似的PES改变(P=0.44)。
观察期间无种植体脱落,达到存留率100%。 3名患者有种植体周围感染,此3名患者均因无足够骨量而接受过引导骨组织再生手术(GBR)。因此,生物学并发症率为7.9%。 2名患者经过刮治后有了很大的改善,1名患者颊侧正中粘膜退缩并且颈部金属暴露。观察期内未发生机械并发症。
表6显示的是从基线到随访1年及2年的临床指标的变化。随时间变化三个指标均未显示出显著差异。牙龈生物型评估得出厚/薄率为28/10。

讨论
本研究用PES/WES评价组织水平种植体周围软组织美学效果及改变。一些研究已经证明了PES/WES指数在临床美学评价方面的可靠性和可重复性(Vilhjalmsson et al.2011; Hof et al.2013)。此外,平均PES改变值也已经被证明适用于评估种植体周围软组织稳定性。 (Cho et al.2010; Dierens et al.2013)。
在本研究中,种植体肩台位置位于对侧牙釉牙骨质界根方1mm。种植体位置对于种植美学效果有着很重要的影响,这也许是本研究两年随访得到的令人满意的平均PES/WES值(7.71/7.25)的原因。 Mangano等在26名单牙缺失患者的美学区即刻植入以莫氏锥度为连接方式的种植体(Leone implant System, Florence,Italy)(Mangano et al.2012),经过2年的随访检查,平均PES/WES值为14.30(7.30/7.00)。 Buser等在20名患者的美学区植入骨水平种植体(Buser et al.2009),在1年随访检查时,平均PES/WES值为16.75(8.10/8.65)。我们的研究表明,在精确控制种植体植入深度的前提下,软组织水平种植体系统在修复单牙缺失病例中也可能会有令人满意的短期美学效果。
种植牙冠外形以WES值来评估。修复体形态、轮廓、颜色、质地、透光度这些参数被分别评估。 WES值(>7)表明修复体美观已经达到。由于WES值在很大程度上与修复设计和质量有关,所以我们更关注PES值。
在本研究中,为了避免冠就位所产生的压力带来的干扰,我们于戴牙2天后获取基线数据。我们观察到1年随访的时候平均PES值较基线有自然的提高,而在第二年的时候这种提高变缓了。
在观察期内,近远中龈乳头高度显著提高。这项观察结果也许是因为被纳入患者为单牙缺失,缺牙间隙旁相邻天然牙有相对较高的骨水平。因为种植支持的修复体其周围龈乳头的丰满程度主要取决于邻牙的骨水平,这是目前呼声很高的观点(Chow & Wang2010; Singh et al.2013)。
观察期内软组织弧度评分也有显著的提高。已有文献证实种植体周围软组织在基台与冠连接后仍在进行改建(Priest 2003; Schropp et al. 2005)。软组织压力随时间得到释放之后也许会变得相对更成熟更健康。这也就解释了为什么软组织弧度评分显著增加。
观察期内软组织边缘水平,根方突度/颜色/质地没有显著差异。甚至在比较2年与1年随访后,软组织边缘水平得分略微下降。这一结果,与我们先前用同一系统种植体的研究有一点点的不同(Lai et al.2008)。在那项研究中,我们纳入的患者都有足够的骨量,在6~8月的随访中软组织边缘水平有显著提高。种植体周围感染导致的3名患者颊侧正中粘膜退缩可以解释这两项研究结果的不同。这与以前文献中报道过的植骨患者有较高的生物学并发症发生率的结果是一致的(den Hartog et al.2013; Santing et al.2013)。
本研究的38个患者中, 24人接受了植骨手术和同期种植体植入术。在基线及后期随访中,植骨患者的平均PES值均显著低于未植骨患者。这表明植骨手术可能对种植体周围软组织的美学效果有不利影响。不利的术前的条件,额外的手术程序所造成的瘢痕组织,较高的并发症发生率以及植骨材料的吸收都可能是造成这一结果的原因。
然而,本研究中不论患者是否有进行GBR手术,都具有相类似的平均PES值变化,植骨患者的2年随访期,平均PES值从5.92上升到7.31。这也表明,在进行过GBR手术的患者中,软组织水平种植体周围软组织美观也有自发改善。
有人认为一段式组织水平种植体周围的生物学宽度较两段式骨水平种植体更接近于天然牙(Hermann etal.2001)。在骨水平种植体系统中必然有基台的断开和再连接,这也许会妨碍结缔组织与种植体之间的相互作用并导致结缔组织更向根方生长(Degidi et al.2011)。此外,最近刚发表的研究报道,组织水平种植体也许较骨水平种植体在长期保持种植体周围骨水平方面更具优势(Chiapasco et al. 2014)。这也许就解释了我们中研究得出的令人满意的结果,并证明了软组织水平种植体也适用于美学区单颗种植牙的修复。
一些研究已经证明了厚龈具有更低的颊侧正中龈缘及龈乳头退缩风险(Lee et al. 2011; Cabello et al.2013)。在本项研究中,厚龈和薄龈生物型患者在基线水平具有相似的PES均值。 2年后随访发现,厚龈型患者相比薄龈生物型患者其种植体周围软组织达到了更令人满意的美学效果。这也就是说,牙龈生物型可以考虑成为美学效果预后影响因素。
除了平均值以外,现存的各特征指数也应当单独用频率进行分析(Lang & Zitzmann 2012)。值得一提的是, PES/WES指数应当被分类为分级数据而不是连续数据。反应离散分布数据的频率分析对于分级数据是重要的 (Shi et al. 2014)。在本研究中,好级在第二年随访的时候几乎是基线时的13倍,不理想级在2年随访后下降。频率分析也证实了美学效果的提高。
结论
本研究结果表明,在美学区用组织水平种植体修复单牙缺失病例是可行的。不论植骨与否,种植体单冠修复周围美学效果和软组织稳定性在短期之内都可以达到满意的结果。然而,植骨手术也许对美学效果有不利影响。牙龈生物型也许可以被认为是影响美学效果预后的因素。组织水平种植体系统对种植体周软组织稳定性的影响,还需要长时间随访的临床随机对照试验提供证据。
鸣谢
We would like to thank Sheng-hui Li (Shanghai Jiao tong University, College of Medicine) for statistics consultation.
参考文献
Al-Nsour, M.M., Chan, H.L. & Wang, H.L. (2012) Effect of the platform-switching technique on preservation of peri-implant marginal bone:a systematic review. International Journal of Oral Maxillofacical Implants 27: 138–145.
Annibali, S., Bignozzi, I., Cristalli, M.P., Graziani, F., La Monaca, G. & Polimeni, A. (2012) Periimplant marginal bone level: a systematic review andmeta-analysis of studies comparing platform switching vs. conventionallyrestored implants. Journal of Clinical Periodontology 39: 1097–1113.
Belser, U., Buser, D. & Higginbottom, F. (2004) Consensus statements andrecommended clinical procedures regarding esthetics in implant dentistry.International Journal of Oral Maxillofacical Implants 19(Suppl): 73–74.
Belser, U.C., Grutter, L., Vailati, F., Bornstein, M.M., Weber, H.P. & Buser, D.(2009) Outcome evaluation of early placed maxillary anterior single-toothimplants using objective esthetic criteria: a cross-sectional, retrospectivestudy in 45 patients with a 2- to 4-year follow-up using pink and whiteesthetic scores. Journal of Periodontology 80: 140–151.
Buser, D., Chappuis, V., Bornstein, M.M., Wittneben, J.G., Frei, M. & Belser, U.C. (2013) Longterm stability of contour augmentation with earlyimplant placement following single tooth extraction in the esthetic zonea prospective, cross-sectional study in 41 patients with a 5- to 9-year follow-up. Journal of Periodontology 84: 1517–1527.
Buser, D., Halbritter, S., Hart, C., Bornstein, M.M., Grutter, L., Chappuis, V.& Belser, U.C. (2009) Early implant placement with simultaneous guidedbone regeneration following single-tooth extraction in the esthetic zone:12-month results of a prospective study with 20 consecutive patients.Journal of Periodontology 80: 152–162.
Buser, D., Martin, W. & Belser, U.C. (2004) Optimizing esthetics for implantrestorations in the anterior maxilla: anatomic and surgical considerations.International Journal of Oral Maxillofacical Implants 19(Suppl): 43–61.
Buser, D., Wittneben, J., Bornstein, M.M., Grutter, L., Chappuis, V. & Belser, U.C. (2011) Stability of contour augmentation and esthetic outcomesof implant-supported single crowns in the esthetic zone: 3-year results ofa prospective study with early implant placement postextraction. Journalof Periodontology 82: 342–349.
Cabello, G., Rioboo, M. & Fabrega, J.G. (2013) Immediate placement andrestoration of implants in the aesthetic zone with a trimodal approach:soft tissue alterations and its relation to gingival biotype. Clinical OralImplants Research 24: 1094–1100.
Chang, M., Wennstrom, J.L., Odman, P. & Andersson, B. (1999) Implantsupported single-tooth replacements compared to contralateral naturalteeth. Crown and soft tissue dimensions. Clinical Oral Implants Research10: 185–194.
Chiapasco, M., Casentini, P. & Zaniboni, M. (2014) Implants in reconstructed bone: a comparative study on the outcome of straumann(R) tissue leveland bone level implants placed in vertically defcient alveolar ridges treated by means of autogenous onlay bone grafts. Clinical Implant Dentistryand Related Research 16: 32–50.
Cho, H.L., Lee, J.K., Um, H.S. & Chang, B.S. (2010) Esthetic evaluation ofmaxillary single-tooth implants in the esthetic zone. Journal of Periodontal Implant Science 40: 188–193.
Chow, Y.C. & Wang, H.L. (2010) Factors and techniques influencingperi-implant papillae. Implant Dentistry 19: 208–219.
Cosyn, J., De Bruyn, H. & Cleymaet, R. (2013) Soft tissue preservation andpink aesthetics around single immediate implant restorations: a 1-yearprospective study. Clinical Implant Dentistry and Related Research 15:847–857.
Cosyn, J., Eghbali, A., De Bruyn, H., Dierens, M. & De Rouck, T. (2012)Single implant treatment in healing vs. healed sites of the anterior maxilla:an aesthetic evaluation. Clinical Implant Dentistry and Related Research14: 517–526.
Degidi, M., Nardi, D. & Piattelli, A. (2011) One abutment at one time:non-removal of an immediate abutment and its effect on bone healingaround subcrestal tapered implants. Clinical Oral Implants Research 22:1303–1307.
Dierens, M., de Bruecker, E., Vandeweghe, S., Kisch, J., de Bruyn, H. &Cosyn, J. (2013) Alterations in soft tissue levels and aesthetics over a 16-22 year period following single implant treatment in periodontally-healthypatients: a retrospective case series. Journal of Clinical Periodontology40: 311–318.
Furhauser, R., Florescu, D., Benesch, T., Haas, R., Mailath, G. & Watzek, G.(2005) Evaluation of soft tissue around single-tooth implant crowns: thepink esthetic score. Clinical Oral Implants Research 16: 639–644.
den Hartog, L., Raghoebar, G.M., Slater, J.J., Stellingsma, K., Vissink, A.& Meijer, H.J. (2013) Single-tooth implants with different neck designs:a randomized clinical trial evaluating the aesthetic outcome. Clinical Implant Dentistry and Related Research 15: 311–321.
Hermann, J.S., Buser, D., Schenk, R.K., Schoolfeld, J.D. & Cochran, D.L.(2001) Biologic width around one- and two-piece titanium implants. Clinical Oral Implants Research 12: 559–571.
Hof, M., Pommer, B., Strbac, G.D., Suto, D., Watzek, G. & Zechner, W.(2013) Esthetic evaluation of single-tooth implants in the anterior maxillafollowing autologous bone augmentation. Clinical Oral Implants Research 24(Suppl A100): 88–93.
Jung, R.E., Pjetursson, B.E., Glauser, R., Zembic, A., Zwahlen, M. & Lang,N.P. (2008) A systematic review of the 5-year survival and complicationrates of implant-supported single crowns. Clinical Oral Implants Research19: 119–130.
Lai, H.C., Zhang, Z.Y., Wang, F., Zhuang, L.F., Liu, X. & Pu, Y.P. (2008)Evaluation of soft-tissue alteration around implant-supported single-toothrestoration in the anterior maxilla: the pink esthetic score. Clinical OralImplants Research 19: 560–564.
Lang, N.P., Zitzmann, N.U. & Working Group 3 of the, V. E. W. o. P. (2012)Clinical research in implant dentistry: evaluation of implant-supportedrestorations, aesthetic and patient-reported outcomes. Journal of ClinicalPeriodontology 39 (Suppl 12): 133–138.
Lee, A., Fu, J.H. & Wang, H.L. (2011) Soft tissue biotype affects implantsuccess. Implant Dentistry 20: e38–e47.
Mangano, F., Mangano, C., Ricci, M., Sammons, R.L., Shibli, J.A. & Piattelli, A. (2012) Singletooth Morse taper connection implants placed in freshextraction sockets of the anterior maxilla: an aesthetic evaluation. ClinicalOral Implants Research 23: 1302–1307.
Mombelli, A., van Oosten, M.A., Schurch, E., Jr & Land, N.P. (1987) Themicrobiota associated with successful or failing osseointegrated titaniumimplants. Oral Microbiology and Immunology 2: 145–151.
Muller, H.P., Heinecke, A., Schaller, N. & Eger, T. (2000) Masticatory mucosa in subjects with different periodontal phenotypes. Journal of ClinicalPeriodontology 27: 621–626.
Pieri, F., Aldini, N.N., Marchetti, C. & Corinaldesi, G. (2013) Esthetic outcome and tissue stability of maxillary anterior single-tooth implants following reconstruction with mandibular block grafts: a 5-year prospectivestudy. International Journal of Oral Maxillofacical Implants 28: 270–280.
Pjetursson, B.E., Bragger, U., Lang, N.P. & Zwahlen, M. (2007) Comparisonof survival and complication rates of tooth-supported fxed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). ClinicalOral Implants Research 18(Suppl 3): 97–113.
Pjetursson, B.E., Thoma, D., Jung, R., Zwahlen, M. & Zembic, A. (2012) Asystematic review of the survival and complication rates of implant-supported fxed dental prostheses (FDPs) after a mean observation period ofat least 5 years. Clinical Oral Implants Research 23(Suppl 6): 22–38.
Priest, G. (2003) Predictability of soft tissue form around single-tooth implant restorations. International Journal of Periodontics Restorative Dentistry 23: 19–27.
Santing, H.J., Raghoebar, G.M., Vissink, A., den Hartog, L. & Meijer, H.J.(2013) Performance of the Straumann bone level implant system for anterior single-tooth replacements in augmented and nonaugmented sites:a prospective cohort study with 60 consecutive patients. Clinical OralImplants Research 24: 941–948.
Schropp, L., Isidor, F., Kostopoulos, L. & Wenzel, A. (2005) Interproximalpapilla levels following early vs. delayed placement of single-tooth implants: a controlled clinical trial. International Journal of Oral Maxillofacical Implants 20: 753–761.
Shi, J.Y., Wang, R., Zhuang, L.F., Gu, Y.X., Qiao, S.C. & Lai, H.C. (2014)Esthetic outcome of single implant crowns following type 1 and type 3implant placement: a systematic review. Clinical Oral Implants Research26: 768–774.
Singh, V.P., Uppoor, A.S., Nayak, D.G. & Shah, D. (2013) Black triangle dilemma and its management in esthetic dentistry. Dental Research Journal(Isfahan) 10: 296–301.
Vilhjalmsson, V.H., Klock, K.S., Storksen, K. & Bardsen, A. (2011) Aesthetics of implant-supported single anterior maxillary crowns evaluatedby objective indices and participants’ perceptions. Clinical Oral ImplantsResearch 22: 1399–1403.
Weinlander, M., Lekovic, V., Spadijer-Gostovic, S., Milicic, B., Wegscheider,W.A. & Piehslinger, E. (2011) Soft tissue development around abutmentswith a circular macro-groove in healed sites of partially edentulous posterior maxillae and mandibles: a clinical pilot study. Clinical Oral ImplantsResearch 22: 743–752.